

Divorce and Health Insurance: What Happens to Your Coverage in 2026
Divorce ends the coverage you carried on a spouse's plan — usually within 30 days of the decree. For healthy, higher-income professionals who don' qualify for subsidies, a private medically underwritten PPO often costs far less than COBRA, with nationwide access and year-round enrollment.
Private PPO • Individual Coverage • Compare Plans
Divorce and Health Insurance: What Happens to Your Coverage in 2026
When exactly does your coverage end?
If you were the spouse carried on the other's employer or individual plan, divorce removes you as an eligible dependent. In most cases coverage ends on the last day of the month the divorce is finalized — though the exact date can be set by your decree or your plan administrator. Confirm it in writing so you know your real cutoff.
Your options after divorce
- Keeps the exact same plan, doctors, and network
- No health screening required
- Available for up to 36 months after divorce
- You pay the full premium — your share plus the employer's
- Often $500–$900+/month for one adult
- Most expensive route for a healthy person
- Best value if your employer covers 70%+ of premium
- Losing spousal coverage is a qualifying event to enroll
- Pre-existing conditions covered — no underwriting
- Only an option if your job offers benefits
- Enroll within your employer's election window (often 30 days)
- Guaranteed issue — covers any health history
- Losing coverage = 60-day Special Enrollment Period
- Subsidies possible only if income is below the threshold
- Higher earners pay the full unsubsidized rate
- Often HMO/EPO — regional networks
- Premium based on your health and age — not your income
- Nationwide PPO — see any participating doctor, no referrals
- $0 and low-deductible options available
- Available any month — no enrollment window
- For healthy applicants, often less than COBRA
- Health questionnaire required — not for every health history
Why a private PPO often fits higher-income professionals after divorce
If you're self-employed, a business owner, or simply earn above the subsidy threshold, the ACA marketplace charges you the full unsubsidized rate — and COBRA charges you the entire group premium. Neither is priced in your favor.
A private medically underwritten PPO is priced on your health and age instead of your income, so a healthy applicant frequently lands below both COBRA and unsubsidized ACA for comparable or broader coverage. And because it's a nationwide PPO with no referrals, it travels with you — useful if your work, your kids, or your post-divorce life now spans more than one state.
- Healthy, no major chronic conditions or ongoing specialty care
- Income above the ACA subsidy threshold (or variable self-employed income)
- Self-employed, business owner, or higher-earning professional
- Want nationwide coverage rather than a regional HMO/EPO network
Don't forget the kids
If your children were covered on the plan you're losing, they need a coverage plan too. Typically the parent providing coverage per the divorce decree enrolls them — through their own employer plan, the ACA marketplace, or a family private PPO. Coordinate this with your decree so there's no lapse and no duplication.
What coverage actually costs after divorce
Here's a realistic comparison for a healthy 45-year-old non-smoker with no major health history, in Florida or Texas — two of our most common markets:
COBRA (ex-spouse's plan)
- $500–$900+/mo for one adult
- Same plan and doctors
- Up to 36 months
- Full group premium + admin fee
- Most expensive for healthy people
ACA Marketplace (unsubsidized)
- Silver: $560–$720/mo
- Gold: $680–$860/mo
- Subsidies only below income threshold
- Often regional HMO/EPO networks
- Income reconciliation at tax time
Private Medically Underwritten PPO
- Often $300–$500/mo for a healthy 45-year-old
- Nationwide PPO — no referrals
- $0 deductible options available
- Not income-dependent — no reconciliation
- Available any month
*Estimates based on 2026 market data for healthy non-smokers in FL and TX. Actual figures vary by age, state, plan, health history, and underwriting outcome.
How to time the switch with no gap
30–45 days before coverage ends
- Confirm your exact coverage end date in writing
- Get pre-screened for private PPO eligibility
- Compare COBRA cost, ACA estimate, and private PPO side by side
At and after the decree
- 60-day special enrollment window opens when coverage ends
- COBRA can serve as a short backstop if underwriting is still processing
- Private plan effective the 1st of the following month — no gap if timed right
We compare COBRA, ACA, and private PPO for your exact situation — and pre-screen private eligibility before you apply. No pressure, no obligation.
Frequently Asked Questions
When does my coverage on my spouse's plan actually end?
In most cases it ends on the last day of the month the divorce is finalized, though your decree or plan administrator may set a different date. Confirm the exact cutoff in writing with the plan administrator so you can line up replacement coverage with no gap.
Is divorce a qualifying event for new coverage?
Yes. Losing coverage due to divorce triggers a 60-day Special Enrollment Period on the ACA marketplace, and it's also a qualifying event to join your own employer's plan (usually within about 30 days). Private medically underwritten PPO plans don't require a qualifying event at all — they're available any month.
How long can I keep COBRA after a divorce?
Divorce is a qualifying event that allows the former spouse to elect COBRA for up to 36 months. The trade-off is cost: you pay the full group premium plus a small administrative fee, which is why COBRA is often the most expensive option for a healthy person.
Will my income from the divorce affect ACA subsidies?
Possibly. ACA subsidies are based on Modified Adjusted Gross Income, and a settlement or change in income can move you above or below the threshold. Tax treatment of support payments depends on when your agreement was finalized. Work with your CPA on the numbers — and note that a private PPO is priced on health, not income, so it sidesteps this entirely.
What about coverage for my kids?
If your children were on the plan you're losing, the parent responsible for their coverage under the decree enrolls them — through an employer plan, the ACA marketplace, or a family private PPO. Coordinate it so there's no lapse and you're not paying for duplicate coverage.
What if I have a health condition and don't qualify for a private plan?
If private underwriting isn't available based on your health history, COBRA and the ACA marketplace remain solid options — the ACA is guaranteed issue regardless of health. We compare all three honestly and tell you which fits before you apply for anything.
Independent broker. We run COBRA, ACA, and private PPO side by side for your situation. Free quotes, honest advice, no pressure.
Robert Adams * President & Licensed Agent * NPN 19540130 * Licensed in 30 states. Premium estimates are illustrative ranges based on 2026 market data and are not guaranteed. Actual premiums vary by age, state, tobacco status, plan selection, carrier, and underwriting outcome. Private medically underwritten plans are not ACA-compliant and are subject to medical underwriting — not all applicants qualify. COBRA timelines and costs vary by plan; coverage end dates vary by decree and plan administrator. This content is for informational purposes only and does not constitute insurance, legal, tax, or financial advice — consult your attorney and CPA for your specific situation.
GLP-1 Coverage Explained: Ozempic, Wegovy & Zepbound in 2026
Whether a plan covers a GLP-1 usually comes down to what it's prescribed for. Diabetes use is commonly covered; weight-loss coverage in 2026 is limited, shrinking, and almost always tied to prior authorization. Here's how each coverage path works — and what to check before you enroll.
Prescription Drug Coverage • Compare Plans • Health Insurance Tips
GLP-1 Coverage Explained: Ozempic, Wegovy & Zepbound in 2026
First, what counts as a "GLP-1"?
GLP-1 receptor agonists mimic a hormone that helps regulate blood sugar and appetite. The brand names get used interchangeably in the headlines, but the FDA approvals behind them are different — and that difference drives whether your plan pays.
Approved for type 2 diabetes
- Ozempic (semaglutide)
- Mounjaro (tirzepatide)
- Rybelsus (oral semaglutide)
- Trulicity, Victoza
Approved for chronic weight management
- Wegovy (semaglutide)
- Zepbound (tirzepatide)
- Saxenda (liraglutide)
The 2026 coverage picture, by plan type
| Coverage path | For diabetes / cardiac use | For weight loss alone |
|---|---|---|
| ACA Marketplace plans | Commonly covered, often with restrictions | Rarely covered — and declining |
| Employer plans | Commonly covered | Only if the employer buys a weight-management rider |
| Private PPO plans | Varies by formulary — verify the drug list | Often excluded or on a high specialty tier |
| Medicare Part D | Covered for approved non-weight uses | Limited — see the GLP-1 Bridge note below |
Why weight-loss coverage keeps shrinking
At roughly $1,000+ per month at list price, GLP-1s have become one of the fastest-growing line items in pharmacy budgets — and insurers have pointed to them as a factor pushing 2026 marketplace premiums higher. The result: many carriers have narrowed weight-loss coverage to diabetes-only, added prior authorization, or dropped it entirely for individual and small-group members effective January 2026.
What this means for you
- A plan covering Ozempic for diabetes may not cover Wegovy for weight loss.
- Even "covered" weight-loss prescriptions usually need prior authorization first.
- Coverage can change at renewal — what's on the formulary this year may shift next year.
If a plan does cover it: how approval usually works
When a plan includes weight-loss GLP-1s, approval criteria tend to mirror the FDA prescribing guidelines:
Typical approval requirements
- BMI of 30+, or 27+ with a weight-related condition (high blood pressure, prediabetes, high cholesterol)
- A documented diagnosis with the correct code from your provider
- A prior authorization request submitted by your prescriber
- In some plans, step therapy — trying a lower-cost option first
Good to know
- Prior authorization can take up to 10 business days
- Ask your prescriber's office to submit it the day the script is written
- Denials can be appealed — and appeals succeed more often than people expect
If your plan excludes it: lower-cost paths
A coverage denial isn't a dead end. Several manufacturer and pharmacy programs exist for people paying out of pocket:
Manufacturer direct
- NovoCare (Wegovy): injection from about $199/month for new patients, then higher; Wegovy pill from about $149/month
- LillyDirect (Zepbound): from about $299/month depending on dose
Pharmacy savings
- GoodRx and similar tools for semaglutide and tirzepatide pricing
- Commercial-insurance copay cards
- Manufacturer cards exclude government plans (Medicare/Medicaid)
A new Medicare GLP-1 Bridge program begins July 1, 2026, giving eligible Part D beneficiaries access to certain weight-loss GLP-1s for a $50 monthly copay through the end of 2027, with prior authorization and clinical criteria required. This applies to Medicare members specifically — separate from the under-65 coverage this guide focuses on.
What to check before you enroll in any plan
- Pull the plan's drug formulary and search the exact brand you take
- Review the Summary of Benefits and Coverage (SBC) — every plan must provide one
- Confirm the tier and whether prior authorization or step therapy applies
- Check whether coverage is tied to a diabetes diagnosis or includes weight management
Where we come in
- We'll run this formulary check with you before you commit to a plan
- Compare your options side by side across carriers
- No surprises at the pharmacy counter
- Free, and no obligation
We'll review the drug lists with you and compare your options side by side — at no cost.
Frequently Asked Questions
Is Ozempic covered by health insurance?
Ozempic is FDA-approved for type 2 diabetes (and cardiovascular risk reduction in certain adults with diabetes), so it's commonly covered when prescribed for those uses — often with prior authorization. It is not FDA-approved as a weight-loss drug, so plans generally won't cover it for weight loss alone.
Why would my plan cover Ozempic but not Wegovy?
They share the same active ingredient (semaglutide) but have different FDA approvals. Ozempic is approved for diabetes; Wegovy is approved for weight management. Formularies follow the approved use, so a plan can include one and exclude the other.
Do ACA Marketplace plans cover GLP-1s for weight loss?
Rarely in 2026. Industry analyses found only about 26 of roughly 300 marketplace carriers cover GLP-1s for obesity, concentrated in nine states, and coverage has been declining. Plans that do cover them typically require prior authorization or quantity limits. Always check the specific plan's formulary.
What if my prescription is denied?
Denials can often be appealed, and appeals succeed more often than people expect — many simply never file one. You can also use manufacturer direct programs and pharmacy savings tools while you sort out coverage. Your prescriber's office handles the prior authorization and appeal paperwork.
Can a private PPO plan get me GLP-1 coverage?
It depends entirely on the individual plan's formulary. Private PPO drug lists vary, and weight-loss GLP-1s are often excluded or placed on a high specialty tier. The reliable move is to verify the exact medication on the formulary before you enroll — which is something we can do with you directly.
We're an independent broker. We'll check the formulary, compare carriers, and tell you honestly what each plan covers for your situation. No pressure, no obligation.
Robert Adams * President & Licensed Agent * NPN 19540130 * Licensed in 30 states. This content is for informational purposes only and does not constitute insurance, medical, legal, tax, or financial advice. Prescription coverage, formularies, prior-authorization rules, and manufacturer program pricing vary by plan, state, and date and change frequently — verify details against your plan's current formulary and Summary of Benefits and Coverage, and consult your healthcare provider about any medication. Private medically underwritten plans are not ACA-compliant and are subject to medical underwriting — not all applicants qualify.
Summer Insurance Shock: Are Teachers Paying COBRA-Level Premiums?
Many teachers assume their "district health insurance" is a great deal — but family premiums often rival COBRA costs. For healthy families, moving dependents to a private PPO while keeping the teacher on the district plan can save $500–800/month
insurance Tips • Compare Plans • Private PPO
Summer Insurance Shock: Are Teachers Paying COBRA-Level Premiums?
The hidden cost of "district insurance"
Most teachers know their district contributes toward health insurance. What many don't realize is how that contribution is structured — and how little of it applies to family coverage.
According to the National Council on Teacher Quality (NCTQ), districts cover an average of 84% of employee-only premiums but only 64% of family premiums. The gap between those two numbers is where teachers get hit.
The result: a teacher paying $162/month for single coverage might pay $711/month or more for family coverage — a jump that rivals what they'd pay on COBRA.
Why family premiums are so high
Employee-only coverage
- District pays 80–90% of premium
- Teacher pays $100–200/month
- Feels like a "great benefit"
Family coverage
- District contribution doesn't scale proportionally
- Teacher picks up most of the dependent cost
- $600–900+/month is common
- Some districts exceed $1,000/month
In Texas specifically, the state contributes just $75/month toward employee coverage, plus a $150/month district minimum. That's $225/month total — for the teacher only. Family members? That's on you.
The split coverage strategy
Here's what some teachers are doing instead: keep the employee on the district plan (to capture the employer contribution), and move spouse and kids to a private medically underwritten PPO.
- Teacher stays on district plan — low cost, good coverage
- Dependents move to private PPO — often $400–600/month for spouse + kids
- Total family cost drops by $500–800/month in many cases
- Private plan has nationwide PPO network (UHC Choice Plus)
- No enrollment window — available any month
- Before: $780/month (district family plan)
- After — Teacher: $19/month (district employee-only)
- After — Spouse + 2 kids: $521/month (private PPO)
- New total: $540/month
- Savings: $240/month ($2,880/year)
Who this works for — and who it doesn't
Good candidates for split coverage
- Healthy spouse and children
- No major chronic conditions or ongoing specialty care
- Family members rarely use the healthcare system
- Current family premium exceeds $600/month
Not a fit if
- Spouse or child has significant health history
- Pre-existing conditions that require ongoing care
- Mental health or substance abuse treatment is needed
- You need guaranteed-issue coverage regardless of health
What private PPO coverage looks like
UnitedHealthcare Choice Plus PPO — Secure Advantage
- $0 day-to-day deductible — benefits start immediately
- 6 prepaid doctor visits per person/year
- $10 generic / $40 brand prescriptions
- Unlimited telehealth included
- $2,500–$10,000 deductible options for major medical
- 80/20 coinsurance up to max out-of-pocket
- Guaranteed renewable to age 65
What's not covered
- Inpatient mental health treatment
- Drug and alcohol rehabilitation
- Pre-existing conditions (underwriting required)
If these exclusions are a concern, district or ACA marketplace coverage may be the better path.
We'll compare your district family plan vs. employee-only + private PPO for dependents — and tell you honestly which path saves more.
How to know if this makes sense for you
Step 1 — Check your current family premium
- Look at your district benefits statement
- What are you actually paying for employee + dependents?
- Is your total above $600/month?
Step 2 — Get a private quote for dependents
- We'll run numbers for spouse and kids on a private PPO
- Based on their ages, ZIP code, and health profile
- Takes about 5 minutes
Step 3 — Compare total costs
- District employee-only + private PPO for dependents
- vs. district family plan
- The math tells you whether it's worth it
Step 4 — Pre-screen for underwriting
- Before applying, we check whether your family members are likely to qualify
- No surprises
- Honest assessment before you commit
Frequently Asked Questions
Does this work during the school year or only in summer?
Private PPO plans are available any month — no enrollment window. You can make the switch whenever your district's open enrollment allows you to drop dependents from the district plan.
What if my district requires me to cover my spouse?
Most districts don't require dependent coverage — it's optional. Check your benefits handbook or HR department. If coverage is truly required, this strategy won't work.
Can I add my kids back to the district plan later if needed?
Typically yes — during the next open enrollment period, or if you have a qualifying life event (job loss, birth, etc.). Confirm with your district's HR.
What if my spouse doesn't qualify for private coverage?
If underwriting isn't available for your spouse due to health history, they can stay on the district plan or explore ACA marketplace options. We compare all paths honestly.
Does this affect my pension or retirement benefits?
No. Your employment status and pension contributions are separate from which health plan your dependents use.
The bottom line
Not every teacher is overpaying for family coverage — but many are. If your district family premium is $600/month or more and your dependents are healthy, it's worth running the numbers on a split coverage strategy.
We'll compare your district family plan vs. employee-only + private PPO for dependents — and tell you honestly which makes sense.
Get a free comparison — your district plan vs. private PPO options for your family.
Robert Adams * President & Licensed Agent * NPN 19540130 * Licensed in 32 states. Premium estimates are illustrative and based on general market data — actual premiums vary by age, state, health profile, and underwriting outcome. Private medically underwritten plans are not ACA-compliant and are subject to medical underwriting — not all applicants qualify. District plan costs vary significantly by state and district. This content is for informational purposes only and does not constitute insurance, legal, tax, or financial advice.
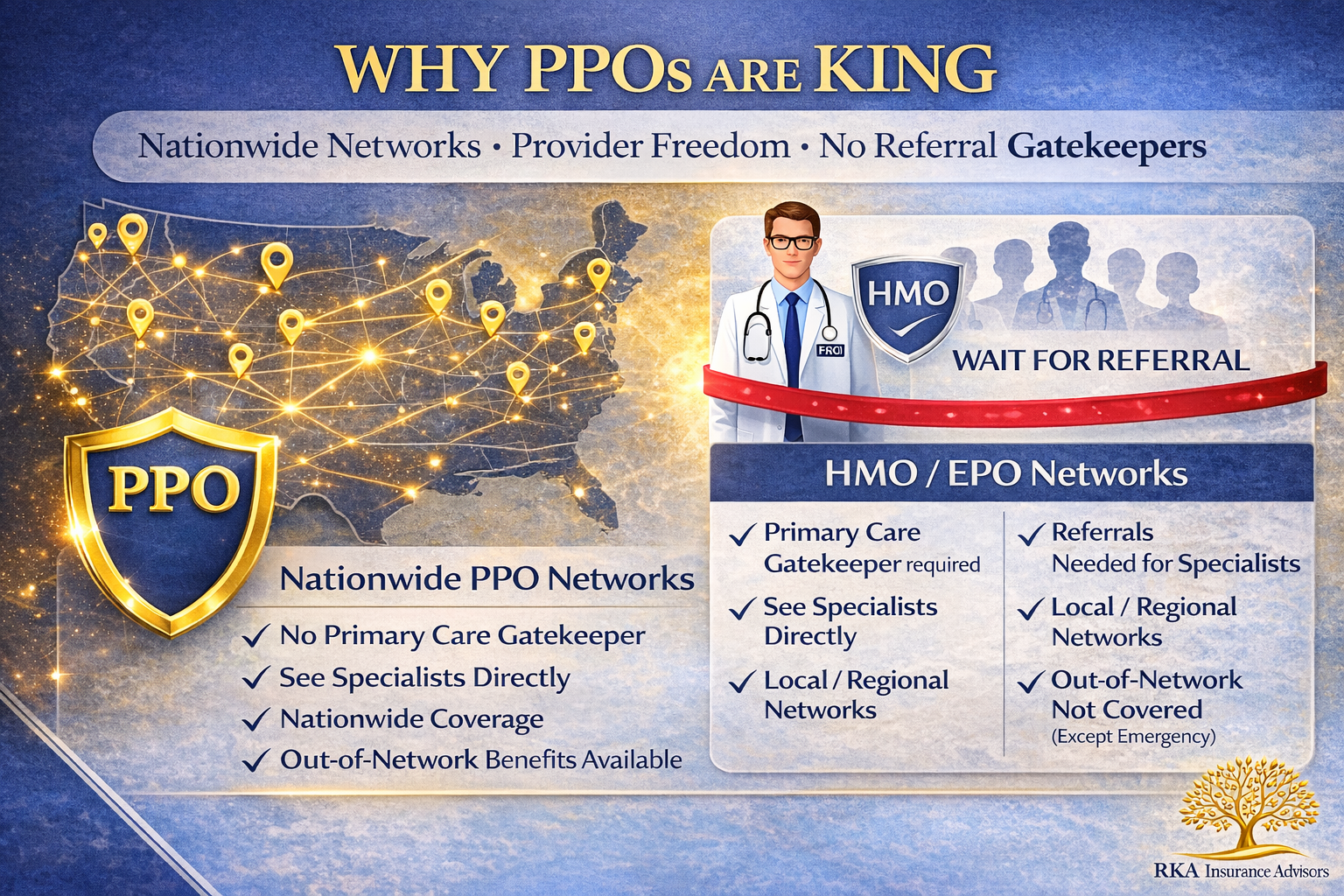
Why PPOs Are King: The Case for Nationwide Networks and Provider Freedom
Why PPOs beat HMOs for self-employed professionals, business owners, and frequent travelers: nationwide networks, no primary care gatekeepers, direct specialist access, and fewer authorization delays.
Why PPOs Are King: The Case for Nationwide Networks and Provider Freedom
Fast take: If you're self-employed, travel for work, or value direct access to specialists without referral red tape, PPO networks offer unmatched flexibility. No primary care gatekeepers, no waiting weeks for authorization, and coverage that works wherever you are—not just in your home county.
Tired of narrow HMO networks and referral requirements?
We'll show you nationwide PPO options and verify your doctors are covered—no restrictions, no runarounds.
Get Free Quotes Book a CallWhat makes PPO networks different
HMO/EPO (Most Marketplace plans)
✗ Primary care doctor required (PCP)
✗ Referrals needed for specialists
✗ Limited to local network only
✗ Out-of-network = not covered (except emergencies)
✗ Authorization delays common
PPO (Preferred Provider Organization)
✓ No primary care gatekeeper required
✓ See specialists directly—no referrals
✓ Nationwide network coverage
✓ Out-of-network benefits available
✓ Fewer authorization requirements
Who benefits most from PPO networks
Business owners & entrepreneurs
✓ Client meetings across multiple states
✓ Need care wherever business takes you
✓ Can't afford delays waiting for referrals
✓ Want specialist access without bureaucracy
Frequent travelers
✓ Snowbirds splitting time between states
✓ Digital nomads working remotely
✓ Families with second homes
✓ Need consistent coverage anywhere
People with specific provider needs
✓ Established relationship with specialist
✓ Prefer specific hospitals or facilities
✓ Need access to top-tier medical centers
✓ Don't want to change doctors
High-income households
✓ Don't qualify for meaningful ACA subsidies
✓ Paying full price either way
✓ Want maximum flexibility and choice
✓ Prefer premium networks and providers
Real-world scenarios where PPOs win
Scenario 1: The entrepreneur in pain
HMO path: Back pain → see PCP first → wait for referral → wait for specialist appointment → weeks of delays
PPO path: Back pain → call orthopedist directly → appointment this week → faster treatment
Scenario 2: The traveling consultant
HMO path: Urgent care needed in Dallas → not in network → pay full cost out-of-pocket → file claim, hope for reimbursement
PPO path: Urgent care in Dallas → nationwide network → normal copay → done
Scenario 3: The specialist relationship
HMO path: Your cardiologist isn't in network → forced to switch doctors → rebuild relationship from scratch
PPO path: Your cardiologist is in nationwide PPO → keep your doctor → continuity of care
Scenario 4: The imaging authorization
HMO path: Doctor orders MRI → need authorization → wait 5-7 business days → delay diagnosis
PPO path: Doctor orders MRI → schedule immediately → faster diagnosis and treatment
The hidden costs of HMO restrictions
Many people choose HMOs to save on monthly premiums, but the total cost equation includes more than just what you pay each month:
Time costs
✗ Waiting for PCP appointments before specialist referrals
✗ Authorization delays (5-7 days common for imaging/procedures)
✗ Extended treatment timelines due to referral requirements
✗ Lost productivity from delayed care
Out-of-pocket surprise costs
✗ Traveling for work? Out-of-network urgent care = full cost
✗ Emergency room in another state = potential balance billing
✗ Preferred specialist not in network = start over with new doctor
✗ Lab work at non-contracted facility = surprise bills
PPO networks for self-employed professionals
If you're self-employed, your health insurance needs are different from W-2 employees:
You can't afford downtime
No paid sick leave. Every day you're delayed waiting for referrals or authorizations is lost income. PPOs let you see specialists immediately and get treatment faster.
Your work location varies
Client sites, conferences, remote work from different states—you need coverage that travels with you, not just in your home county.
You control your own schedule
Don't waste time scheduling PCP visits just to get a referral. See the specialist directly and get back to work.
You're paying full freight anyway
If you don't qualify for subsidies, you're paying full price for ACA plans. PPO premiums are often comparable with far better access.
Common PPO myths debunked
❌ Myth: PPOs are always more expensive
Reality: For healthy applicants who don't qualify for subsidies, private underwritten PPOs often cost less than unsubsidized ACA plans—with better networks and lower deductibles.
❌ Myth: You don't need nationwide coverage
Reality: Even if you rarely travel, emergencies happen. Car accident on vacation? Family emergency out of state? Nationwide PPO coverage eliminates surprise bills.
❌ Myth: Referrals aren't a big deal
Reality: Referral requirements add 1-3 weeks to every specialist visit. For time-sensitive issues or busy professionals, this delay is costly.
❌ Myth: All PPOs are the same
Reality: PPO network size varies dramatically. We verify your specific doctors are in-network before you enroll—not all "nationwide" PPOs include every provider.
When to choose PPO over HMO/EPO
Choose PPO if...
✓ You're self-employed or own a business
✓ You travel frequently for work or personal reasons
✓ You have established relationships with specialists
✓ You don't qualify for meaningful ACA subsidies
✓ You value direct access without referral delays
✓ Time is money and you can't afford bureaucratic delays
HMO/EPO might work if...
✓ You qualify for strong ACA subsidies
✓ All your doctors are in a local HMO network
✓ You rarely travel and don't need out-of-area care
✓ You're comfortable with PCP gatekeeping
✓ You don't mind waiting for referrals and authorizations
✓ Lowest monthly premium is your only priority
How RKA finds the right PPO for you
Doctor verification first
We check your specific doctors, specialists, and hospitals against actual PPO networks—not just "find-a-doc" directories that are often outdated.
Multi-state coverage mapping
Travel between Florida and New York? We verify both locations have strong network coverage before you commit.
Total cost comparison
We model premiums + deductibles + expected usage for HMO vs PPO options—sometimes PPO costs less when you factor in out-of-network exposure.
Private vs Marketplace PPO options
Marketplace has limited PPO options. We compare against private underwritten PPOs that may offer better networks and lower deductibles.
Ready for nationwide PPO freedom?
We'll verify your doctors, compare PPO options, and show you total costs—no referral requirements, no network restrictions.
Get Free Quotes Book a CallQuick FAQs
Are PPOs available on the ACA Marketplace?
Some states offer limited PPO options on the Marketplace, but many areas only have HMO/EPO plans. Private underwritten PPOs (off-exchange) often offer broader networks and better benefits for healthy applicants.
Do PPOs really cost that much more than HMOs?
For subsidized plans, yes. But if you don't qualify for subsidies, private PPO premiums are often comparable to unsubsidized HMO/EPO plans—with far better access and lower deductibles.
What does "nationwide PPO" actually mean?
Network coverage in all 50 states (or most states). Specific provider availability varies—we verify your doctors are included, not just that the network exists in your state.
Can I switch from HMO to PPO mid-year?
ACA plans can only switch during Open Enrollment (or with a qualifying event). Private PPOs are available year-round if you qualify for underwriting.
For education only; network access and benefits vary by carrier and state. Always verify providers before enrollment. Eligibility for private underwritten plans subject to medical underwriting.